21 April 2024 11:14
Topic starter
5
Why do so many people say they benefited greatly from microdosing, when researchers cannot statistically significantly demonstrate that it is better than a placebo?
5 Answers
6
29 July 2025 15:16
Placebo and nocebo are two powerful psychological mechanisms that can have a direct influence on your physical and mental health. With a placebo effect Positive expectation leads to improvement, even if no active substance is administered. In the case of a nocebo effect The exact opposite happens: negative expectations can cause or worsen physical or psychological complaints — purely based on conviction.
Triptherapie explains in the blog From nocebo to placebo with psychedelic therapy from the fact that these effects are not imagination, but neurologically measurable processes. The stress hormone cortisol plays a key role in this. Negative thoughts increase cortisol, which suppresses the immune system and blocks natural recovery. Positive expectations, on the other hand, do the exact opposite—they activate the body's self-healing capacity.
Psychedelics, such as psilocybin, can help break stubborn nocebo patterns. During a session, it becomes Default Mode Network (DMN) — the brain network that supports self-criticism, rumination, and ingrained beliefs, among other things — is temporarily less active. As a result, old patterns can be released, and new insights and connections emerge. Some participants experience this as a mental reset, in which negative beliefs make way for more compassion and acceptance.
This means that psychedelics are not placebos, but they can activate placebo substitute effect, by helping people open themselves up to healing and change. Moreover, psilocybin stimulates the production of BDNF, a growth hormone that promotes neuroplasticity and enables recovery at a neurological level.
Does microdosing work better than a placebo?
According to Triptherapie, it works microdosing with psychedelics such as psilocybin no better than a placebo with most people. In the article “Macrodosing works better than microdosing” It is explained that the amount of active substance in microdosing is often too small to have an actual effect in the brain. This is partly due to the enzyme MAO (monoamine oxidase), which can rapidly break down psilocybin and psilocin in the body before they can do their job.
Only if you take a dosage that above the threshold depending on your MAO capacity, sufficient psilocin reaches the brain to have a noticeable effect. With microdosing, that usually doesn't happen — and even if it does have an effect once, your body often starts producing more MAO, causing the effect to fail to materialize later on.
Some long-term positive effects of microdosing can be explained by indirect mechanisms, such as improved serotonin synthesis or altered neurochemistry — but these effects are mild and slow. In contrast to microdosing, macrodosing (normal or high dosage) shows much clearer, long-lasting, and measurable effects on, for example, mood, insight, and neuroplasticity.
In short: microdosing acts as a placebo for many people — which can still be valuable. But if you really want therapeutic results, Triptherapie recommends a psilocybin session with an effective dosage, tailored to your neurochemistry and goal. Do you want to know what works best in your situation? Then fill out the intake for tailored advice in.
3
10 February 2026 18:50

We are increasingly discovering that people take doses that are too low when microdosing, or that some tolerance develops over time. As a result, a microdose might not quite work, or it might work, only to subsequently have less effect or do nothing at all due to tolerance. Getting the dosage right is therefore the hardest part; you don't want to take too much or too little. Aside from this, we see more progress with occasional higher doses of psilocybin than with microdosing only with truffles.
3
27 February 2026 13:37
We previously wrote a message stating that microdosing does not work much better than a placebo. You cannot underestimate the effects of the placebo, and this is the biggest reason why microdosing works. If you look beyond the studies and read the positive stories about microdosing psychedelics, it is possible that the researchers are overlooking something.
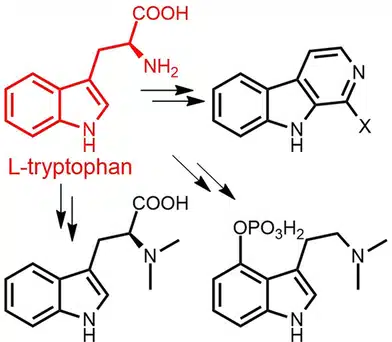
We know that the absorption of tryptophan, the building block of serotonin, is difficult and barely reaches the brain. Psilocin (from truffles), however, enters the brain very easily if you take the threshold level into account. Now, tryptophan and psilocin are closely related since tryptophan is the precursor of psilocin. It is possible that you even convert oxidized psilocin in the brain into a building block for serotonin, which in turn could be positive for mood in the long run. This could then explain the long-lasting positive effects without microdosing having much influence in the short term.
Please note: This is a theory that still needs to be scientifically investigated. The current state of affairs:
Limited absorption of tryptophan. The essential amino acid l-tryptophan is used only in small quantities for the synthesis of serotonin; most intake is converted via the kynurenine pathway.. Moreover, the transport capacity across the blood-brain barrier is limited and depends on the ratio of tryptophan to other large neutral amino acids..
Psilocin is lipophilic and crosses the BBB easily. Psilocybin is converted in the body to psilocin, which is lipophilic thanks to an intramolecular hydrogen bond.. As a result, psilocin has little trouble passing the BBB, and the effect sets in quickly. So, this is indeed much easier than with serotonin.
Similar breakdown pathways of psilocin and serotonin. Both psilocin and serotonin are oxidized by MAO to hydroxyindole-3-acetaldehyde and subsequently to hydroxytryptofol or hydroxyindole-3-acetic acid.. This underscores the biochemical relationship between both molecules.
No evidence that psilocin metabolites serve as serotonin precursors. Although psilocin is related to tryptophan and serotonin, there is no scientific evidence that the metabolite 4‑HIAA or other oxidized psilocin derivatives are converted back to serotonin or tryptophan in the brain. The metabolites are largely excreted in the urine. and 5‑HIAA, the analog serotonin metabolite, barely crosses the BBB.
Long-term mood improvements caused by psilocybin likely occur via other mechanisms. Studies report that psilocybin has long-lasting antidepressant effects.. These effects are likely caused by long-term receptor agonism, neuroplasticity, and interactions with the gut microbiome., not by the recycling of psilocin metabolites into serotonin.
In summary: The theory that oxidized psilocin can be converted into building blocks for serotonin in the brain currently finds no support in the scientific literature. However, research shows clear differences in the availability of tryptophan and psilocin to the brain and great similarities in their degradation. The long-term positive effects of psilocybin are likely due to receptor agonism and neuroplasticity, not to direct serotonin replenishment via psilocin metabolites.
Source: Microdosing might actually work
2
19 February 2026 17:44
More and more people are foregoing microdosing and opting for a higher-dose psychedelic trip. This is because the BDNF-increasing properties are absent or negligible with microdosing. This has been proven at higher doses. Reducing inflammation also works better at higher doses.
1
4 March 2026 11:30
To substantiate this discussion with the current state of scientific knowledge, we delve into the results of clinical studies and neurological research. This makes the gap between the user's "experience" and the scientist's "data" much clearer.
1. The "Self-Blinding" study (Szigeti et al., 2021)
This is one of the largest and most cited studies on microdosing. Because lab studies are expensive and strictly regulated, researchers from Imperial College London had 191 users make their own capsules (placebo vs. microdose) via an ingenious "blind" system.
-
The finding: After four weeks, the microdosers reported significant improvements in well-being and less anxiety. However, the group that thought they were taking a microdose but actually took a placebo showed exactly the same improvements.
-
Conclusion: The positive effects of microdosing are likely a result of expectation (expectancy effect) and not of the pharmacological effect of the substance at that low dose.
2. Neuroplasticity and BDNF
BDNF is being discussed on the forum (Brain-Derived Neurotrophic Factor), a protein that is essential for the repair and growth of neurons.
-
High dosage: It has been irrefutably proven that a "macrodose" (a full trip) causes a massive spike in BDNF and a temporary increase in neural connections. We call this the "window of plasticity".
-
Microdosing: In human studies, the evidence for an increase in BDNF with microdosing is very weak. In animal studies (in rats), some change is observed, but humans have a much more complex metabolism and a different density of the -receptors.
-
The threshold value: Scientists suspect that there is a threshold at which the The receptor must be sufficiently stimulated to initiate the signal cascade for BDNF. A microdose often falls short of this.
3. The role of the -receptor
Psychedelics act primarily on serotonin -receptor.
-
At a full dose, approximately 60% to 80% of these receptors in the cortex occupied. This leads to the mystical experiences and the therapeutic breakthroughs.
-
With a microdose, the occupancy is likely less than 10% to 20%. Many researchers doubt whether this is enough to bring about a lasting change in brain structure without the help of the placebo effect.
4. Why does it work "intuitively" after all, then?
Scientists are looking at two factors that can complement the forum theory about "building blocks":
-
Subtle cognitive shifts: Some lab studies (including from Maastricht University) found that microdosing improves focus and "divergent thinking" (creativity). something improved, but only in specific tasks. The effect is so small that in daily life it is hardly distinguishable from a good cup of coffee or a day with high self-confidence.
-
Low-grade anti-inflammatory: There is growing interest in the anti-inflammatory properties of psychedelics. Even a microdose could theoretically reduce minor inflammation in the brain, producing a mild antidepressant effect, independent of the "trip".
In summary: Science vs. Practice
Science currently says: "We do not see the effects that users claim reflected in the data once we add a placebo." The theory on the forum that psilocin crosses the blood-brain barrier more easily than tryptophan is correct, but the assumption that it is subsequently "recycled" into serotonin currently lacks biological evidence. Most psilocin simply leaves the body via urine.