
Topic starter
Who a ceremony or considering a psilocybin session and taking an SSRI at the same time Those who use them often receive conflicting information. In one place it says the combination is not possible, in another it says they work perfectly fine together. The reality lies somewhere in between. Pharmacologically, truffles and magic mushrooms involve the same family of psychoactive substances, namely psilocybin and psilocin, so the core question is primarily how an SSRI can affect the experience and the tapering process.
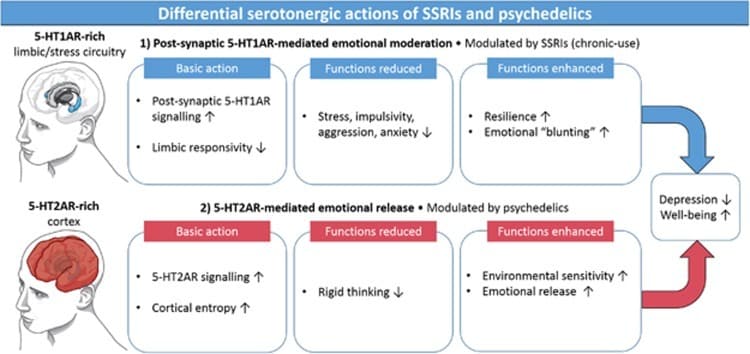
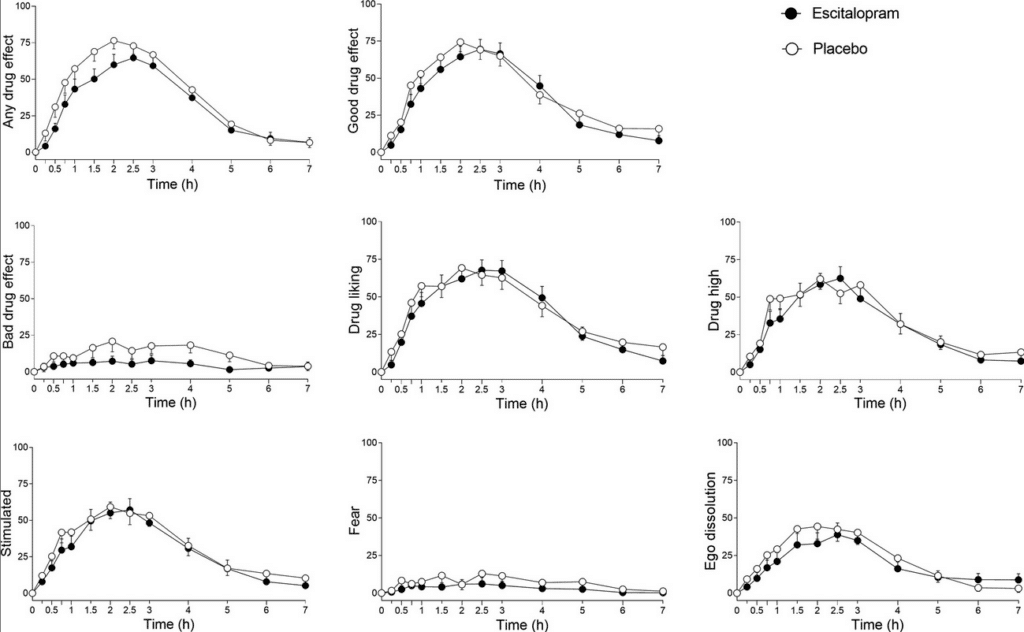
What we now know from research and clinical observations is that psilocybin in combination with an SSRI is not by definition impossible or acutely unsafe, but that the experience can turn out differently. In a controlled study with escitalopram, the positive mood effects of psilocybin remained largely present, while anxiety, adverse effects, and some physical side effects were actually lower. At the same time, a later analysis showed that stopping SSRIs or SNRIs beforehand does not automatically lead to a better treatment outcome, and that tapering itself can also be a confounding factor.
Therefore, in practice, there are usually three routes. The first route is to continue using the SSRI and still schedule the session. The second route is to taper off more quickly and then wait until approximately five times the half-life has passed. The third route is to taper off more gradually, then stabilize, and only perform a session when withdrawal symptoms have truly disappeared. The exact duration depends on the substance, the dose, the duration of use, age, liver function, susceptibility to withdrawal, and the psychological stability at that moment. The time estimates below are therefore practical plans for ceremony preparation, not official medical tapering schedules.
Spoiler
Fluoxetine, Prozac and Sarafem
Fluoxetine, Prozac and Sarafem
Fluoxetine is the SSRI where time requires the most attention. The half-life of fluoxetine itself is approximately 4 to 6 days with chronic use. In addition, the active metabolite norfluoxetine remains present for much longer, with a half-life that is around 9.3 days in older label information and is described as even longer in other official information. As a result, fluoxetine can continue to affect the serotonergic system for weeks, even after a person has stopped taking it.
With option 1, i.e., continued use, the fastest route is usually that preparation can start within about 1 to 2 weeks and the session can be scheduled relatively quickly thereafter. The advantage is that you do not induce a withdrawal phase. The disadvantage is that fluoxetine can flatten the intensity of the psilocybin experience and that, due to its long duration of action, this drug is also difficult to “just” bypass.
With option 2, i.e., tapering off faster and then waiting, fluoxetine is the slowest SSRI of them all. Five times the half-life of fluoxetine alone amounts to approximately 20 to 30 days. If you also take norfluoxetine into account, that waiting period can practically run towards 47 days. Including an accelerated tapering, a ceremony plan therefore often ends up taking about 4 to 8 weeks, and sometimes longer.
With option 3, i.e., tapering off gradually and then stabilizing, it is more realistic to think in terms of several months. For some people, 2 to 4 months can already be tight, especially after long-term use. Particularly with fluoxetine, it makes more sense not only to look at the half-life but also at how long the nervous system needs to feel stable again. That is also the reason why this route often offers the best chance of a psilocybin experience with as little reduction as possible.
Spoiler
Sertraline, Zoloft and Lustral
Sertraline, Zoloft and Lustral
Sertraline has an average terminal half-life of approximately 26 hours. Pharmacologically, therefore, it is cleared from the body much faster than fluoxetine. This makes planning more straightforward, but it still does not mean that someone is immediately clinically ready for a session as soon as the drug has largely disappeared from the blood.
With option 1, continued use, preparation can usually take place within 1 to 2 weeks. This route is practically the fastest, but there remains a chance that the psilocybin experience will be less deep or less pronounced. For some people, this is actually workable, especially if anxiety or restlessness is a major part of their symptoms.
With option 2, tapering off more rapidly and then waiting five times the half-life, purely pharmacologically this results in a waiting period of approximately 5 to 6 days after the last dose. In practice, the tapering itself must be added to this, meaning the total planning often comes to about 2 to 4 weeks. This is a realistic middle ground if the patient does not experience too severe dysregulation upon dose reduction.
With option 3, gradually tapering off and stabilizing, a process of approximately 1 to 3 months is often more realistic. With long-term use or previous withdrawal problems, this may take longer. The advantage of this route is that you run less risk of the session being disrupted by insomnia, anxiety, irritability, or other withdrawal symptoms.
Spoiler
Paroxetine, Paxil and Seroxat
Paroxetine, Paxil and Seroxat
Paroxetine has an average half-life of approximately 21 hours. On paper, this appears to be a drug that is quickly cleared from the body, but in practice, paroxetine is notorious for withdrawal symptoms if you stop too soon. The official product information also explicitly warns against discontinuation syndrome and advises tapering off gradually.
With option 1, continued use, preparation can often start again within 1 to 2 weeks. That is the fastest and sometimes also the least disruptive route. The downside is that the psilocybin effect may be diminished, causing someone to sink less deeply into the material than hoped.
With option 2, tapering off faster and then waiting, based purely on half-life, you arrive at approximately 4 to 5 days after the last dose. However, paroxetine is precisely a medication where that pharmacological calculation tells only part of the story. In practical planning, it is therefore often more realistic to think in terms of about 3 to 6 weeks rather than just a few days plus a mini-tapering.
With option 3, gradually tapering off and stabilizing, a course of approximately 2 to 4 months is often more logical, and sometimes longer. Especially for people who have been using paroxetine for months or years, this is frequently the safest and most comfortable route. It is also often the route with the best chance of performing the ceremony without withdrawal symptoms clouding the experience.
Spoiler
Citalopram, Celexa and Cipramil
Citalopram, Celexa and Cipramil
Citalopram has an average terminal half-life of approximately 35 hours. This places the drug in the middle category in terms of timing. It is not as slow-acting as fluoxetine, but also not as short-acting as fluvoxamine. Abrupt discontinuation is advised against in the official information, because citalopram can also cause significant withdrawal symptoms.
With option 1, continued use, preparation for a psilocybin, truffle, or mushroom session is often possible within 1 to 2 weeks. This is practically attractive and prevents disruption caused by sudden tapering. However, the chance remains that the experience will feel less powerful or less complete.
With option 2, tapering off faster and then waiting, you end up with approximately 7 to 8 days for citalopram at five times the half-life. If you add an accelerated tapering process to that, the total schedule usually comes to around 2 to 4 weeks. For many people, this is the route that feels most feasible, provided they are not too sensitive to withdrawal.
For option 3, gradually tapering off and stabilizing, a window of approximately 1 to 3 months is often a more realistic one. With long-term use, this can increase. This route generally offers the lowest chance that restlessness, insomnia, or dysregulation resulting from the tapering process will carry over into the ceremony itself.
Spoiler
Escitalopram, Lexapro and Cipralex
Escitalopram, Lexapro and Cipralex
Escitalopram has an average half-life of approximately 27 to 32 hours. This is also the SSRI for which we have the most direct experimental information in combination with psilocybin. In the controlled study of escitalopram and psilocybin, the positive mood effects of psilocybin largely persisted, while anxiety and adverse effects actually decreased. This makes escitalopram the SSRI where option 1 is relatively defensible in some cases, provided the rest of the situation is stable.
With option 1, continued use, a preparation of about 1 to 2 weeks is often sufficient. For some people, this is actually the best route, because the risk of withdrawal symptoms is eliminated and the combination does not automatically block the entire experience. However, it remains an individual decision, as not everyone reacts the same way.
With option 2, tapering off more quickly and then waiting, five times the half-life results in approximately 6 to 7 days. Including the tapering itself, this usually means about 2 to 4 weeks in practical planning. This is often feasible with shorter use or when previous dose reductions were well tolerated.
For option 3, gradually tapering off and stabilizing, approximately 1 to 3 months is often more logical. With longer use or sensitivity to dysregulation, this may increase further. This route is usually most suitable if someone wants both as full an experience as possible and a sustainable transition to less or no medication.
Spoiler
Fluvoxamine, Luvox and Faverin
Fluvoxamine, Luvox and Faverin
Fluvoxamine has an average half-life of approximately 15.6 hours in young, healthy adults. In the elderly, this half-life can be significantly longer, up to approximately 17.4 to 25.9 hours depending on the dose and situation. This means that fluvoxamine can be eliminated pharmacologically quite quickly, but also that age is an additional factor to consider in planning.
With option 1, continued use, it still holds true that preparation is often possible within 1 to 2 weeks. The advantage is rest and continuity. The disadvantage is once again that the psilocybin effect may be less pronounced.
With option 2, tapering off more quickly followed by a wait, based purely on half-life, you arrive at approximately 3 to 4 days for younger adults. In practical planning, however, you usually still end up with about 2 to 4 weeks, especially if you want to taper off cautiously or if the person is somewhat older. For the elderly, it is advisable to build in extra margin, as fluvoxamine is demonstrably cleared more slowly in this age group.
For option 3, gradually tapering off and stabilizing, approximately 1 to 3 months is often a workable starting point, and sometimes longer for older users or long-term use. This makes this route particularly interesting when someone is sensitive to anxiety or when the session really only needs to be scheduled once the system feels calm and predictable again.
What is the most logical choice now?
The shortest route is usually option 1, i.e., continued use, with a preparation period of approximately 1 to 2 weeks. The middle route is usually option 2, i.e., faster tapering plus a waiting period, which generally results in 2 to 4 weeks for most SSRIs, except for fluoxetine, where it can take 4 to 8 weeks or longer. The most extensive route is option 3, i.e., gradual tapering and stabilization, for which you should usually expect 1 to 3 months or longer, and often even longer for fluoxetine or paroxetine. These differences are primarily explained by half-life, active metabolites, and the risk of dysregulation during discontinuation.
The most important conclusion, therefore, is not that SSRIs and psilocybin never go together, but that the path must be chosen wisely. Sometimes continued use is the best option. Sometimes tapering off more quickly is sufficient. And sometimes a longer, slower course is actually the most sensible choice. The best decision depends on the specific substance, the dosage, the duration of use, susceptibility to withdrawal, and whether someone primarily wants to have a session quickly or wants the greatest chance of an experience that is as minimally diminished as possible.
Would you like an extra check? Then fill in the intake at Triptherapie and also request information from the doctor who prescribes your medication. This way, every situation can be assessed uniquely!
Spoiler
SSRI and LSD, MDMA, psilohuasca and ayahuasca
Substances such as LSD, MDMA, ayahuasca, psilohuasca, and psiloflora
With LSD, similar interactions are generally assumed as with psilocybin, truffles, and magic mushrooms. Here too, SSRIs can dampen or alter the effects. Therefore, broadly speaking, the same considerations apply regarding continued use, tapering, and stabilization, although the direct modern research literature on LSD is more limited than on psilocybin.
Substances such as MDMA, ayahuasca, psilohuasca, and psiloflora require extra caution when using an SSRI. The information in this article regarding tapering off SSRIs can broadly serve as a starting point for MDMA, ayahuasca, psilohuasca, and psiloflora as well, but with an important difference. Option 1 is not a suitable route in this case. In the case of ayahuasca and psilohuasca (including Chocbliss or Cacao Bliss), this is primarily because these combinations rely on MAO-A inhibition, meaning that concomitant use with SSRIs is considered a significant contraindication due to the risk of serotonergic toxicity and other undesirable interactions. The same applies, to a lesser extent, to psiloflora. We exercise the same caution, as it also contains an MAO-inhibiting component.
Option 2 That could be a possibility, provided that after tapering, not only is approximately five times the half-life taken into account, but also an extra safety margin to account for the fact that degradation and recovery may differ per person. Option 3, So, tapering off gradually, then stabilizing, and only then doing the session is generally the safest option.
Posted : 20 March 2026 10:58