
Topic starter
This new scientific article investigated how intravenous DMT as a bolus injection behaves in the body, how quickly and how strongly the acute psychedelic effects occur, and whether those effects change at different dosages and forms of administration. The work was published on March 27, 2026 in Translational Psychiatry and focuses explicitly on healthy participants, not on patients in therapeutic treatment. The central question was therefore not whether DMT is already effective as a therapy here, but rather what each dose does, how long it lasts, how tolerable it is, and what role expectation, blinding, and dose escalation play in the experience.
What exactly the researchers did
The study consisted of two separate research arms. In the first arm, 20 healthy participants received five administrations in random order on a single test day: placebo and DMT of 5, 10, 15, and 20 mg, double-blind and placebo-controlled. In the second arm, 16 healthy participants received open-label placebo first, followed by ascending doses in 5 mg increments up to a maximum of 25 mg, with participants allowed to decide after each dose whether they wanted to increase the dose further. All boluses were administered intravenously in 20 ml over 45 seconds, with approximately 1 hour between doses.
The participants chose their preferred arm themselves, so they were not randomly assigned to the two arms. This is important because it makes the comparison between the two setups less robust. The researchers measured subjective effects, positive and negative experiences, anxiety, altered consciousness, blood pressure, side effects, and plasma concentrations of DMT up to 55 minutes after each bolus.
The most important outcome in one sentence
The main message of the article is that intravenous bolus DMT acts extremely rapidly and for a short duration, that the peak experience in the randomized double-blind arm showed a kind of ceiling effect around 15 mg, and that open-label dose escalation made the experience clearly more tolerable than unexpected, blinded, random dosing.
How fast DMT worked
DMT worked very quickly in this study. Subjective peak effects were usually reached within 1 to 3 minutes, and in the time measurements, the researchers observed that the strong effects emerged primarily within the first 2 minutes. Afterward, they subsided rapidly. At lower doses, such as 5 and 10 mg, the effects declined quickly after the peak. At higher doses, such as 15 to 25 mg, the effects remained close to peak levels for a few minutes before further diminishing. The total duration of distinct subjective effects ranged from approximately 12 to 30 minutes, depending on the dose.
This makes this form of administration pharmacologically striking. The experience is much shorter than, for example, a classic psilocybin or LSD session, but the onset is much more abrupt and therefore potentially more overwhelming. The authors emphasize that precisely this rapid, intense peak is likely a major reason why bolus DMT can be subjectively less well tolerated than a more gradual continuous infusion.
What the dose did to the intensity
In the double-blind randomized arm, subjective effects increased dose-dependently, and effects were significantly different from placebo starting as early as 5 mg. At the same time, the researchers observed a ceiling effect for peak intensity starting at 15 mg. This does not mean that higher doses had no additional effect, but rather that the maximum peak experience no longer increased proportionally. The duration of the experience did continue to increase, however, and the 20 mg dose resulted in a greater total exposure time than the 15 mg dose.
There is a practically relevant distinction there. A higher dose above 15 mg therefore did not simply result in an “even higher peak,” but rather a slightly longer or heavier burden on the system, with also a greater chance of unpleasant effects. This is important for future clinical dosing policy, because it suggests that there comes a point where further escalation becomes less efficient if your primary goal is a strong peak effect.
Positive and negative effects
Participants generally reported far more positive than negative effects, but negative reactions did increase at higher doses. 15 and 20 mg, in particular, were associated with more “bad drug effect” and “fear”. On broader psychedelic scales, the researchers also observed that higher doses resulted not only in more classic mystical and consciousness-altering effects, but also more anxious ego dissolution, distressing experience, and loss of control.
This makes the study substantively interesting for a therapeutic context. It shows that high intensity does not automatically equate to a better experience. A strong peak can be simultaneously impressive, positive, and frightening. The authors explicitly describe that participants sometimes experienced the first wave of effects at higher doses as simultaneously good, bad, and anxiety-inducing.
Pharmacokinetics: what happened in the blood?
Plasma concentrations of DMT increased approximately dose-proportionally. In the randomized arm, mean Cmax values were around 11, 20, 37, and 45 ng/ml for 5, 10, 15, and 20 mg, respectively. Peak blood concentration was reached after approximately 2.3 to 2.7 minutes. This was followed by a rapid decline, with an early estimated half-life of approximately 6.1 to 6.8 minutes.
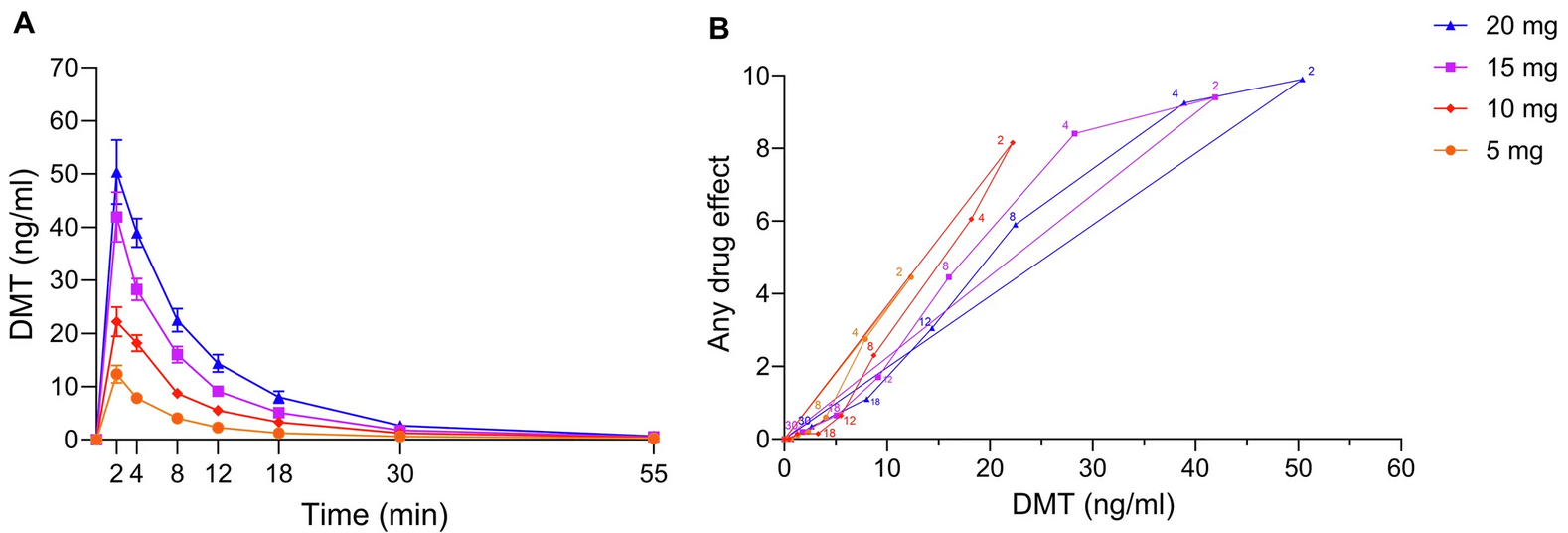
That pharmacokinetic profile fits well with the subjective course. DMT rises very rapidly in the plasma and also falls rapidly again. At the lower doses, 5 and 10 mg, the subjective effects followed blood levels fairly neatly. At 15 and 20 mg, however, the subjective effects remained close to their peak while the plasma concentration was already decreasing. The authors describe this as a form of counterclockwise hysteresis, i.e., a delayed response relative to the blood level. This again supports the idea that you do not simply get a linear increase in peak intensity at higher doses.
Was tolerance built up?
An important result is that the researchers found no acute tolerance with this bolus design. They observed this in two ways. First, the concentration-response relationship showed no pattern indicating rapid flattening of effect during a single dose. Second, assessments of “any drug effect” at equivalent doses were comparable, even with repeated administration at one-hour intervals.
This is relevant because some acute tolerance was indeed described in previous work with continuous DMT infusion. This study therefore suggests that the development of tolerance may depend strongly on the method of administration and/or the dosing course. Short-term intermittent boluses appear to behave differently from longer-term continuous exposure.
Why open-label dose escalation is so important
Perhaps the most interesting part of the article is the difference between the two study designs. In the open-label dose-escalation arm, the same dose levels were systematically perceived as less intense than in the double-blind randomized arm. Positive effects were comparable or linearly increasing, but negative effects, in particular, were clearly lower. The authors report that negative effect ratings in that arm at comparable dose levels were nearly 50% lower. On some scales for total peak experience, positive scores were approximately 50% lower and negative scores even approximately 60% lower than in the randomized arm.
The researchers interpret this as a strong signal that expectation, context, and a sense of control noticeably influence the DMT experience. Those who know what dose is coming, can acclimate step by step, and are allowed to decide for themselves whether to increase the dose, presumably feel safer and less overwhelmed. This could particularly dampen negative reactions such as anxiety and loss of control. This aligns with the broader psychedelic principle of set and setting, but here it becomes very concretely visible in a dosing experiment.
How bearable was it?
Overall, the authors found the tolerability acceptable, despite the intensity. Many participants completed the entire session, even in the randomized arm with multiple boluses in one day. In the open-label arm, 10 of the 16 participants continued to the maximum dose of 25 mg, including three psychedelically naive participants. One participant stopped after 10 mg, three after 15 mg, and two after 20 mg.
However, there were clear physical and psychological stress effects. DMT increased systolic and diastolic blood pressure in a dose-dependent manner. Frequently reported complaints were headache, concentration problems, feelings of weakness, and palpitations. Additionally, one participant experienced anxiety and panic attacks after the session, requiring psychiatric follow-up; these symptoms initially resolved within two months, later returned, and were subsequently treated with psychotherapy and escitalopram.
That last point is important. Although it concerns only one case, it shows that even in a controlled setting with healthy volunteers, an acute DMT experience can have a persistent psychological aftermath. For clinical application, this means that proper screening and aftercare remain essential.
How good was the blackout?
The blinding was only partially effective. Placebo and 5 mg were recognized correctly relatively often, whereas the higher doses after each administration were also frequently misjudged, usually as the adjacent dose. According to the authors, this underscores how difficult it is to maintain truly convincing blinding with strong psychoactive substances. Even an active placebo such as 5 mg DMT may not be sufficient to effectively mask the higher doses. After all, both researchers and participants quickly realize what the possible dose might be.
For psychedelic research, this is methodologically important, because expectations and assumptions about the received dose can themselves influence outcomes. This ties in with the main theme of this article: not only pharmacology, but also the context of administration partly determines how intense and how well tolerated the experience is.
Strengths of the study
The study has a few clear strengths. It used multiple doses in a controlled crossover design, included placebo, took into account both subjective and physiological measures, and provided fairly detailed pharmacokinetic data. Additionally, men and women were equally represented, and standardized psychometric scales were used. The extra open-label dose escalation arm is also a substantively strong addition, as it shows how dosing strategy and expectation context can shift the experience.
Limitations and what you should not conclude from them
The authors themselves mention a number of important limitations. First, participants in the dose escalation arm could drop out prematurely, which may have made the higher dose groups in that arm more selective. Second, participants chose their own arm, making comparisons between the two arms more susceptible to bias. Third, the study was statistically designed primarily for comparisons within each arm, not for drawing firm conclusions between the two arms. And finally, the participants were healthy subjects in a highly controlled setting, meaning the results cannot simply be translated one-to-one to psychiatric patients or therapeutic sessions in practice.
In concrete terms, this means that you should not conclude from this that 15 mg is “the best therapeutic dose,” or that open-label administration is by definition clinically superior. What you can reasonably say, however, is that this study provides good indications regarding acute dose-response, time course, tolerability, and the importance of expectation management.
Substantive interpretation
In terms of content, this is a valuable study because it demonstrates three things simultaneously. First, it confirms that bolus DMT has an ultra-fast and short-acting psychedelic profile. Second, it suggests that with this form of administration, a functional tipping point already exists around 15 mg, where one does not gain more peak intensity linearly, but can experience additional stress. Third, it convincingly shows that control, predictability, and gradual build-up can significantly mitigate the experience, particularly on the negative side.
That is likely the most important lesson for future therapeutic applications of DMT. Not only the molecule and the dose matter, but also how that dose is administered. A protocol involving dose escalation or titration may be clinically more interesting than an abrupt high bolus, precisely because patients may be less likely to become overwhelmed and maintain a greater sense of control. This is not yet proof of better treatment outcomes, but it is a relevant indication for the future design of DMT therapy research.
Shortest conclusion
This article shows that intravenous bolus DMT has a very rapid onset, is short-lived, and increases in potency depending on the dose, but begins to reach a ceiling in terms of peak intensity around 15 mg. Higher doses result in a relatively longer duration and a greater risk of unpleasant effects. At the same time, an open-label, stepwise build-up makes the same substance noticeably more tolerable, likely because control and expectation strongly modulate the experience.
My thoughts on this article
Would a DMT session Would it work better if the active concentration were maintained at a specific level until the therapeutic effect is fully utilized? This would call for a specialized delivery of DMT, where the focus is not on the short and very intense peak, but rather on a more controllable exposure over a longer period. Such an approach might ensure that a person remains in a therapeutically usable state long enough, without repeatedly going through an abrupt and overwhelming peak. This could be therapeutically interesting, as it creates more room for guidance, emotional processing, and targeted interventions during the experience itself.
At the same time, this raises new questions, as it is not yet clear whether the therapeutic value lies primarily in the peak experience, the total duration of the altered state, or the combination of intensity, timing, and psychological support. My preliminary thought is therefore that a more controlled and stable administration of DMT might be more effective in some cases than a short bolus, but that this needs to be thoroughly investigated before firm conclusions can be drawn.
Posted : 1 April 2026 13:15