24 February 2025 20:08
Topic starter
0
How can you compare mescaline to psilocybin?
2 Answers
2
5 March 2025 17:38

Mescaline and psilocybin are both psychedelic substances that can cause powerful consciousness-altering experiences, but they differ in chemical structure, origin, and effects.
Origin and chemical structure:
- Mescaline is a naturally occurring substance found primarily in certain cacti, such as the peyote and San Pedro cactus. Chemically, mescaline is a phenethylamine.
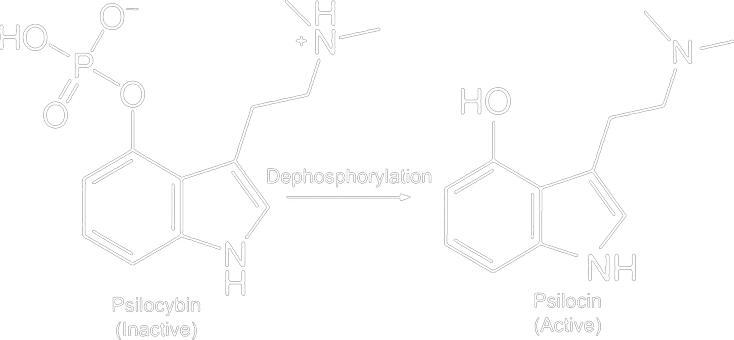
- Psilocybin It occurs in various types of mushrooms, often referred to as 'magic mushrooms' or truffles. After ingestion, psilocybin is converted into psilocin in the body, which causes the psychoactive effects. Psilocybin belongs to the tryptamines.
Effects and duration of action:
Both substances affect serotonin receptors in the brain, leading to altered perceptions, moods, and thoughts. The specific experience may vary depending on the dose, environment, and individual sensitivity. In general, the effects of mescaline last longer (8-12 hours) than those of psilocybin (4-6 hours). Incidentally, mescaline is somewhat comparable to MDMA in combination with truffles (hippieflip).
Therapeutic use:
Psilocybin has received much attention in recent years in scientific research into the treatment of depression, anxiety, and addiction. Mescaline has been less extensively studied for therapeutic purposes, but is traditionally used in certain indigenous cultures for spiritual and healing rituals.
Important consideration:
Combining mescaline with MAO inhibitors can be dangerous and is strongly advised against. MAO inhibitors are sometimes used to enhance the effects of certain psychedelics, but in combination with mescaline, they can lead to serious health risks.
1
5 March 2025 17:47
Introduction: Mescaline and psilocybin are both classic psychedelic substances, but they belong to different chemical classes and have unique backgrounds. Six aspects are compared below: chemical structure, effects, safety, therapeutic potential, historical use, and scientific studies, supported by scientific and historical sources.
1. Chemical Structure
Mescaline: Mescaline (3,4,5-trimethoxyfenethylamine) is a substituted phenethylamine, chemically related to neurotransmitters such as dopamine and noradrenaline. It is a relatively simple molecule with a benzene ring featuring three methoxy groups and an ethylamine side chain. Mescaline belongs to the phenethylamine-class of hallucinogens (such as the 2C-x compounds), sometimes referred to as the “mescaline-like” psychedelics.
Psilocybin: Psilocybin (4-phosphoryloxy-N,N-dimethyltryptamine) is a tryptamine-alkaloid. It has an indole nucleus (related to the structure of serotonin) with a phosphate group at the 4-position. Psilocybin falls into the tryptamine-class of hallucinogens (the “psilocybin-like” psychedelics). In the body, psilocybin is rapidly converted into psilocin (4-hydroxy-DMT), the active form. Both substances – mescaline and psilocybin – are classical serotonergic hallucinogens which derive their effects primarily from agonism of 5-HT2A receptors in the brain.
Chemically, therefore, they differ clearly: mescaline is a relatively simple phenethylamine, while psilocybin is a more complex indole (tryptamine). Despite these structural differences, they belong to the same broad category of psychedelics and cause similar receptor activation in the brain.
2. Effects
Subjective effects: Both substances induce powerful psychedelic experiences (“trips”), with altered perception, emotions, and thoughts. Users of mescaline often report vivid visual hallucinations, such as bright colors, geometric patterns, and a distorted sense of depth and time. Euphoria and a heightened sense of energy may occur, as well as difficulty concentrating and a dreamy mental state. Psilocybin causes similar phenomena: a state of euphoria or wonder, changes in consciousness and perception, and visual and auditory hallucinations (for example, seeing moving patterns or hearing sounds that are not there). Time may feel slowed down or sped up to the user, and ego awareness may diminish, sometimes leading to mystical experiences. Emotionally, psilocybin users may experience deep introspection, sometimes with alternating fits of laughter and moments of fear or insight.
Physiological effects and duration: Mescaline takes on a relatively slow pace: the effects usually start 45–90 minutes after ingestion and can persist for a very long time – often 9 am to 2 pm. In a recent controlled study, the average duration of action of mescaline was measured at approximately 11.1 hours. Psilocybin, on the other hand, takes effect faster: within 20–60 minutes (the effects begin faster when ingested as tea), and these usually last 4–6 hours on. A study reported an average effect duration of ~4.9 hours for psilocybin.
Physiologically, both substances cause mild sympathetic stimulation: dilated pupils, An increased heart rate and blood pressure, and sometimes elevated body temperature and perspiration. Side effects also occur during the trip. Mescaline is known to cause severe nausea and vomiting can cause at the start (something traditionally seen as a cleansing part of the experience). This is sometimes accompanied by dizziness or stomach cramps. Psilocybin can also cause stomach upset, but usually milder; users sometimes report moderate nausea, headache or an unpleasant feeling in the stomach, especially in the initial phase. At high doses or in sensitive individuals, both substances can induce feelings of anxiety during the trip (a “bad trip”), accompanied by panic or confusion. Generally, the acute physical effects are described as non-life-threatening considered and decrease as the psychoactive effect fades.
3. Safety
Toxicity: Mescaline and psilocybin have relatively low physical toxicity. There are no documented deaths due to an overdose of mescaline in human use. The estimate for a lethal dose of mescaline is extremely high – for example, an LD_50 of approx. 880 mg/kg in humans, which amounts to many tens of grams for an adult – hundreds of times higher than a typical dose (~0.3 grams). Psilocybin is also physically very non-toxic: animal studies suggest a lethal dose that approximately 1,000 times higher is then the effective dose. By way of illustration, psilocybin has a therapeutic index (safety margin) of ~641, significantly higher (safer) than, for example, alcohol or nicotine. In practice, a fatal overdose with psilocybin-containing mushrooms is considered extremely unlikely Considered – serious physical consequences occur at most upon ingestion of astronomical quantities. In short, at normal dosages, both substances cause no organ damage and the toxicity is negligible.
Addictive potential: Both psychedelics have a low addiction potential. They do not cause physical dependence; tolerance develops quickly with repeated use, which reduces the effect and discourages frequent abuse. Studies show that repeated use of psilocybin not leads to physical dependence. Mescaline is also widely used not as addictive considered. Unlike, for example, opioids or stimulants, psychedelics do not cause compulsive use—rather the contrary, the often intense and confronting experiences cause users to take breaks of their own accord. Psychic addiction (the craving for the experience) rarely occurs, at most in cases of irresponsible, extreme use. Moreover, there is cross-tolerance: the use of mescaline temporarily reduces sensitivity to psilocybin and LSD, and vice versa, making frequent use even less attractive.
Possible risks: The greatest risks of both mescaline and psilocybin are psychological of a nature. During a “bad trip,” intense fear, paranoid thoughts, or panic reactions may occur, sometimes accompanied by disorientation or brief hallucinations. In most cases, these reactions are temporary and disappear as soon as the effects wear off. Nevertheless, caution is advised: in vulnerable individuals (e.g., those with a predisposition to psychosis), the use of psychedelics can trigger a latent mental disorder. There are isolated reports of acute psychotic behavior, self-harm, or suicidal impulses during a severe confused trip, although this occurs very rarely. Another long-term risk is HPPD (Hallucinogen Persisting Perception Disorder), in which a person may experience visual disturbances ("flashbacks") for weeks or months after use – however, this is a rare complication.
Physically, the risks are limited to the aforementioned side effects (nausea, headache, etc.). There is no withdrawal syndrome after stopping and no demonstrable organic damage. However, with psilocybin in its natural form (mushrooms), a unique danger Emphasized: a mistake while picking. Wild mushrooms can be confused with poisonous species. Inexperienced collectors risk a fatal poisonous mushroom to consume instead of a psilocybin-containing species. This risk is culturally relevant (particularly outside regulated settings). Mescaline is typically obtained from well-known cacti (peyote, San Pedro), making confusion with a deadly species less likely; however, these cacti are sometimes bitter and can cause other discomfort.
Finally, legal and contextual risks must be mentioned: mescaline and psilocybin are illegal in many countries, which makes quality control and dosage determination difficult. Additionally, inexperienced users can endanger themselves in unsafe environments (e.g., in traffic or at high altitudes) while under the influence of hallucinations. Following the principles of “set and setting”—being in a mentally stable state and using in a safe, familiar environment—is crucial to minimize the risks.
4. Therapeutic Potential
After years of stigmatization, the medical world has once again become interested in the therapeutic applications of psychedelics. Psilocybin leads the way in this regard: in clinical trials, psilocybin-assisted therapy has shown promising results for various mental disorders. For example, in 2018, the FDA granted psilocybin the status of “Breakthrough Therapy” awarded for the treatment of treatment-resistant depression, due to exceptional effectiveness in early studies. In multiple double-blind clinical trials with depressed patients (both with severe depression and with anxiety in terminal cancer patients), one or two sessions with psilocybin, in combination with psychotherapeutic counseling, led to rapid and significant reduction of depressive and anxiety symptoms. This improvement often occurred within 1 week stopped and in many cases for months on. Notably, in a small study, psilocybin scored better than a daily antidepressant (escitalopram) in achieving remission in depression. Other studies demonstrate the potential of psilocybin for addiction treatmentsFor example, in alcohol and tobacco addiction, pilot studies achieved high abstinence rates after psilocybin therapy sessions (±80% success in quitting smoking in an open study, according to Johns Hopkins research). Furthermore, psilocybin is being investigated for obsessive-compulsive disorder, post-traumatic stress disorder (PTSD), and cluster headaches. Although these applications are still in research phases, the results indicate broad therapeutic potential. Importantly, psilocybin therapy safe and well tolerated appeared under medical supervision; patients also frequently report positive long-term changes in attitude to life and well-being after such sessions.
Mescaline has been less extensively clinically investigated, but historical and recent evidence also suggests therapeutic value. Indigenous practices already indicated that peyote (mescaline-containing cactus) could play a role in addiction treatmentWithin the Native American Church, ceremonial use of peyote has been reported as a successful support tool against alcoholism. As early as 1974, a case report described the treatment of alcohol addiction with peyote in Navajo patients with positive outcomes. In the 1950s, mescaline was used incidentally in psychiatry to study models of psychosis and possibly for therapy, but systematic clinical research stalled following the prohibitions. Today, mescaline is experiencing a comeback in research settings. Recent surveys among users indicate that mescaline consumption can be associated with long-term improvements in mental health: in a survey of 452 people, approximately two-thirds of respondents with depression, anxiety, PTSD, or drug abuse indicated that their condition improved after their most meaningful mescaline experience (without this necessarily being the intention). Another analysis reports that of the respondents with self-reported depression 86% improvement experienced improvement after mescaline, and in anxiety disorder ~80%. Although these are observational data, it suggests that mescaline can offer profound insights and perspective shifts that prove therapeutically beneficial – comparable to what has been demonstrated for psilocybin.
Organized clinical research with mescaline is in its infancy. Nevertheless, there are developments: a startup (Journey Colab) is developing a synthetic form of mescaline (JOUR-5700) specifically for the treatment of alcohol addiction, including therapy counseling, and is preparing clinical studies. In addition, there is interest in mescaline for the treatment of depression and anxiety; the long operating time This is viewed here as both a challenge (longer sessions required) and potentially an advantage, as prolonged acute effects may lead to a longer therapeutic aftermath.
In summary, psilocybin is currently the frontrunner in clinical research, with multiple phase 2 and phase 3 studies that promising results show effects in depression, anxiety, and addiction. Mescaline's therapeutic potential is once again being recognized, particularly in the fields of addiction treatment and trauma, but has yet to be formally proven in clinical trials. Both substances, provided they are used safely under professional supervision, could new paradigm in psychiatry can herald for conditions where conventional treatments fall short.
5. Historical Use
Mescaline – traditional and cultural: Mescaline occurs naturally in certain cacti and is for millennia used by indigenous cultures in North and South America. Archaeological findings show that peyote-cacti in Mexico for sure 5,700 years ago were already being used ritually. In the pre-Columbian era, various indigenous peoples (such as the Huichol and other groups in central Mexico) used peyote in shamanistic and religious ceremonies, among other things to induce visions and make contact with the spiritual realm. Also in South America, the San Pedro cactus (Echinopsis pachanoi), which contains mescaline, has a long history of use – for example in the Andes of Peru and Ecuador – where it has been considered a sacred plant since antiquity (Huachuma) is used by shamans. During the Aztec Empire, peyote use was widespread in Mesoamerica for religious purposes, but the Spanish conquistadors oppressed this “pagan” practice was fiercely suppressed in the 16th century. Spanish missionaries banned ritual intoxicants and drove the use of peyote underground. Nevertheless, the use of peyote persisted in remote areas and within indigenous communities. In the late 19th century, peyote began a new chapter in North America: around 1880, a prayer ceremony involving peyote emerged among the Kiowa and Comanche peoples, which led to the establishment of the Native American Church (NAC) early 20th century. The NAC integrated peyote as a sacrament into a Christian-Native American faith synthesis. In 1920, this religious peyote practice became legally recognized in the US (and since 1994 explicitly protected at the federal level for Indigenous communities). Today, mescaline in the form of peyote is still central to NAC ceremonies, which have spread from Mexico to Canada.
In a Western context, mescaline first came to attention with the rise of toxicology and ethnobotany in the 19th century. German researchers isolated mescaline in 1896 (Arthur Heffter identified the alkaloid from peyote) and in 1919 it was first synthesized in the lab (Ernst Späth). Psychiatric pioneers in the early 20th century experimented with it to investigate hallucinations. A famous cultural-historical moment was in 1954, then writer Aldous Huxley described his experience with 400 mg of mescaline in the essay “The Doors of Perception”, in which he took readers along into the vivid hallucinations and profound thoughts evoked by the drug. Huxley's account popularized mescaline in intellectual circles. In the 1960s, mescaline (primarily in the form of dried peyote “knots” or synthetically) became one of the psychedelics adopted by the counterculture. Along with LSD and psilocybin, mescaline emerged in hippie culture as a means of spiritual exploration. However, legal measures in the late 1960s (including the US Controlled Substances Act of 1970) also made mescaline illegal, causing regular use and research to decline sharply. Nevertheless, mescaline retained a respected place in history: on the one hand as entheogen sacrament among indigenous peoples, on the other hand as a source of inspiration in Western art (Huxley, the music of The Doors who took their name from his book) and the burgeoning psychedelic science of the mid-20th century.
Psilocybin – traditional and cultural: Psilocybin is found in so-called “magic mushrooms” (hallucinogenic mushrooms), which have a rich tradition of use in various cultures. Particularly in Mesoamerica This practice dates back a long way. The Aztecs and related Nahua peoples in central Mexico were familiar with hallucinogenic mushrooms as teōnanācatl, literally “divine mushroom” (teōtl = divine, nanācatl = mushroom in Nahuatl). These were used in religious and divination rituals. According to chronicles, such mushrooms were served to guests at the inauguration ceremony of the Aztec Emperor Montezuma II in 1502. The Aztecs believed that teonanácatl enabled the consumer to communicate with the divine or spirit world. In addition to the Aztecs, indigenous groups in Oaxaca (such as the Mazatecs, Mixtecs, and Zapotecs) also traditionally used psilocybin-containing mushrooms in healing rituals and shamanistic ceremonies. The Spanish missionaries forbade However, after the conquest (1520s), all this indigenous hallucinogenic use ceased. Colonial accounts (for example, that of Fray Bernardino de Sahagún) describe how the Spaniards viewed mushroom practices as diabolical and fiercely suppressed them. Despite this, the use persisted. continue living underground in remote regions – small indigenous communities continued to use the “sacred mushrooms” in their traditional rites. This living tradition came to light again for the rest of the world in the mid-20th century: in 1955 were ethnomycologists R. Gordon Wasson and his wife Valentina the first Westerners to participate in a Mazatec nocturnal mushroom ceremony led by shamans (such as María Sabina). Wasson published a famous article about this. “Seeking the Magic Mushroom” in Life magazine (1957), which aroused enormous Western interest. Shortly thereafter, the French mycologist Roger Heim identified the species (Psilocybe mexicana) and in 1958 isolated the Swiss chemist Albert Hofmann the active substances psilocybin and psilocin from these mushrooms. Sandoz Laboratories even briefly marketed a pure psilocybin preparation (“Indocybin”) for research purposes in the early 1960s.
In the 1960s psychedelic mushrooms began to play an important role in the emerging hippie counterculture. Psychologists Timothy Leary and Richard Alpert (Harvard) experimented with psilocybin in the famous Harvard Psilocybin Project (1960–1962), investigating its effects on prisoners and students (with mixed results). Although these studies were controversial—Leary and Alpert were fired in 1963 partly because of this—they contributed to the popularization of psilocybin. In the late 1960s, ’magic mushrooms,“ along with LSD, became icons of the hippie movement, symbols of consciousness expansion and protest against the established order. However, just as with mescaline and LSD, the backlash in the late 1960s led to criminalization: psilocybin was banned internationally in 1970 (UN treaty), and with it, it faded back into the margins until the 21st century.
Culturally, psilocybin mushrooms have left their mark both traditional (as a sacrament among the Mazatecs, for example, where they were called “the flesh of the gods”) as pop culture (in Western art and music, and more recently in the festival/psychonaut scene). Nowadays, we see a renewed interest in traditional practices: tourists travel to Mexico to participate in indigenous ceremonies, while conversely, Western scientists are also integrating the insights of shamans into therapies. In summary, psilocybin has an ancient history as a sacred substance in Native American rituals, a period of discovery and abuse in the West during the 20th century, and a current rehabilitation as a potential medicine.
6. Scientific Studies
Revival of research: After decades of stagnation since the 1970s, there has been a strong revival in scientific research into psychedelics. Mescaline and psilocybin are both the subject of recent studies, although psilocybin has been studied much more intensively to date. Current scientific studies focus on the pharmacology, neurological effects and therapeutic application of these substances.
Pharmacology and mechanism: Research has confirmed that both mescaline and psilocybin derive their psychedelic effects primarily from activation of the serotonin 5-HT2A receptor in the cerebral cortex. This mechanism – shared by all classic hallucinogens – initiates a cascade of changes in neural networks that lead to the characteristic changes in consciousness. Despite the fact that mescaline and psilocybin differ chemically, their pharmacodynamics Thus, largely similar. However, there are nuances: mescaline, for example, also has affinity for certain other receptors (such as 5-HT_1A and adrenergic α_2A), whereas psilocybin's active metabolite psilocin is structurally close to the neurotransmitter serotonin and has a slightly different receptor profile. These small pharmacological differences are being investigated to understand whether they cause subtle variations in effect.
Neurological effects: Modern techniques such as fMRI and EEG are used to map the influence of psychedelics on the brain. Studies with psilocybin show that its use leads to reduced activity and connectivity in the Default Mode Network (DMN) – a brain network involved in self-reflection and basal resting-state activities. This is associated with the letting go of the ego sense and the experience of “oneness” that users often describe. Furthermore, research suggests that psilocybin the release of glutamate increases in certain brain regions and possibly lowers inflammatory markers in the brain, which may contribute to antidepressant effects. In cell and animal studies, it has been observed that psychedelics (including psilocybin) the neural plasticity increase – for example, an increase in dendritic connections (“neural growth”) – which offers a possible explanation for the long-lasting positive effects on mood after only one or two doses. Mescaline has been studied less with neuroimaging, but as a classic psychedelic, it is expected to have similar network effects to psilocybin and LSD. EEG study Studies in rats showed that psilocin, LSD, mescaline, and a related substance (DOB) all caused broadband desynchronization of brain waves and functional decoupling in networks, which corresponds to the disruption of normal patterns of brain activity. However, solid comparative neurostudies in humans are still lacking for mescaline.
Comparative studies: An important question is to what extent different psychedelics various subjective experiences bring about. For a long time, there were mainly anecdotes about this, but recently a direct scientific comparison has been made for the first time. In 2023 became a randomized double-blind crossover study published in which mescaline, psilocybin, and LSD were administered to subjects in equivalent doses, with placebo control. The results are illuminating: Mescaline had the longest duration of effect (average ~11 hours), compared to ~5 hours for psilocybin (LSD was in between with ~8 hours). As for the subjective experience the researchers found, however no qualitative differences between the states of consciousness induced by mescaline and psilocybin when the intensity was comparable. In other words: the nature of hallucinations, the feeling of euphoria or introspection, and scores on psychological scales of altered consciousness were largely the same for psilocybin and mescaline, if the dose was adjusted so that both were equally “strong”. This suggests that our brains respond to these substances in a similar way, despite chemical differences. However, mescaline appeared to be slightly more aftermath side effects to cause (such as fatigue or headache the next day) than psilocybin, possibly due to its longer duration of action. Such studies help debunk myths that certain psychedelics are inherently “friendlier” or “more intense”—it largely comes down to dosage and set/setting. Naturally, there are individual variations; ongoing research attempts to determine whether, for example, personality or genetics causes someone to respond better to one trip or another.
Clinical and therapeutic studies: As described in Section 4, psilocybin is the subject of numerous clinical trials for various indications. A overview of 2024 inventoried 11 clinical trials (of which 5 RCTs) into psilocybin for depression. These broadly confirm that supervised psilocybin therapy significant and long-lasting can alleviate symptoms in depression and anxiety, even in difficult cases (e.g., terminal cancer patients who benefited for >6 months). Phase 3 studies are currently underway to confirm whether psilocybin-assisted therapy is sufficiently safe and effective to become a standard medicine. Mechanisms are also being further unraveled – from neurobiology to the role of the “mystical experience” as a potential mediator of clinical outcome. Clinical research for mescaline is emerging. In addition to the aforementioned comparative study in Basel, a separate dose-escalation study also started there to better establish the safety range of mescaline in humans. The results of this will provide insight into optimal dosages for therapy. Furthermore, case studies and retrospective surveys (such as those published in 2021) are revealing that mescaline possible beneficial effects has for example PTSD and addiction, which can form the basis for future clinical trials.
Trend and future: Scientifically, the attitude towards psychedelics has shifted radically from taboo to curiosity. Major medical journals are now publishing studies on psilocybin (e.g. New England Journal of Medicine, 2022) and there is an increasing number of academic centers and startups worldwide involved in psychedelic research. Scientists do emphasize the need for careful and transparent research, given past mistakes. Currently (2025), dozens of trials are underway with psilocybin, as well as with LSD, MDMA (for PTSD, phase 3), and other entheogens. Mescaline research remains somewhat more of a niche, but its unique position—one of the oldest known hallucinogens, with a rich cultural history and some pharmacological peculiarities—is generating renewed attention. If these studies are successful, psilocybin (and perhaps later mescaline analogues) could be used in the near future as regulated therapies can be used for, for example, depression, anxiety disorders, or addiction, under controlled conditions. This marks a remarkable scientific Renaissance of remedies that were once associated only with counterculture and shamans, but are now (re)finding their place in medicine in an evidence-based manner.
Conclusion: Although mescaline and psilocybin differ in origin and chemistry, they exhibit remarkable similarities in their effects and safety. Both are powerful, non-addictive psychedelics with a relatively safe physical profile. Culturally, they have been used for centuries (if not millennia) as spiritual sacraments. Scientific research, after a long hiatus, confirms many of their similar mechanisms of action and unravels their potential to treat persistent mental disorders. Psilocybin currently holds the lead in this regard, with broad clinical interest and impressive study results, while mescaline—the “forgotten” psychedelic—is beginning to come back into the spotlight thanks to new comparative studies and initiatives in addiction treatment. The comparison between these two substances highlights how diverse the family of hallucinogens is, and at the same time how consistent their core mechanisms of action and—provided they are used carefully—are. value can be, both for science and for different cultures.
Sources: The above analysis is based on a range of scientific publications, traditional reports and modern research results, including pharmaceutical and anthropological literature, to paint an integrated picture of mescaline and psilocybin regarding each of the requested aspects. These sources include both peer-reviewed studies and historical documentation to substantiate the claims and provide context.